Hypertension: The recommended starting dose of valsartan is 80 mg once daily.
The antihypertensive effect is substantially present within 2 weeks, and maximal effects are attained within 4 weeks. In some patients whose blood pressure is not adequately controlled, the dose can be increased to 160 mg and to a maximum of 320 mg. valsartan may also be administered with other antihypertensive agents. The addition of a diuretic such as hydrochlorothiazide will decrease blood pressure even further in these patients.
Recent myocardial infarction: In clinically stable patients, therapy may be initiated as early as 12 hours after a myocardial infarction. After an initial dose of 20 mg twice daily, valsartan should be titrated to 40 mg, 80 mg, and 160 mg twice daily over the next few weeks. The starting dose is provided by the 40 mg divisible tablet.
The target maximum dose is 160 mg twice daily. In general, it is recommended that patients achieve a dose level of 80 mg twice daily by two weeks after treatment initiation and that the target maximum dose, 160 mg twice daily, be achieved by three months, based on the patient's tolerability. If symptomatic hypotension or renal dysfunction occur, consideration should be given to a dose reduction.
Valsartan may be used in patients treated with other post-myocardial infarction therapies, e.g. thrombolytics, acetylsalicylic acid, beta blockers, statins, and diuretics. The combination with ACE inhibitors is not recommended.
Evaluation of post-myocardial infarction patients should always include assessment of renal function.
Heart failure: The recommended starting dose of valsartan is 40 mg twice daily. Up titration to 80 mg and 160 mg twice daily should be done at intervals of at least two weeks to the highest dose, as tolerated by the patient.
Consideration should be given to reducing the dose of concomitant diuretics. The maximum daily dose administered in clinical trials is 320 mg in divided doses.
Valsartan may be administered with other heart failure therapies. However, the triple combination of an ACE inhibitor, a beta blocker and valsartan is not recommended. Evaluation of patients with heart failure should always include assessment of renal function.
Additional information on special populations: Elderly: No dose adjustment is required in elderly patients.
Renal impairment: No dose adjustment is required for adult patients with a creatinine clearance >10 ml/min.
Hepatic impairment: Valsartan is contraindicated in patients with severe hepatic impairment, biliary cirrhosis and in patients with cholestasis. In patients with mild to moderate hepatic impairment without cholestasis, the dose of valsartan should not exceed 80 mg.
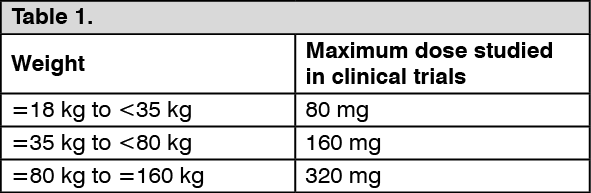
Paediatric population: Paediatric hypertension: Children and adolescents 6 to 18 years of age: The initial dose is 40 mg once daily for children weighing below 35 kg and 80 mg once daily for those weighing 35 kg or more. The dose should be adjusted based on blood pressure response. For maximum doses studied in clinical trials refer to the table as follows.
Doses higher than those listed have not been studied and are therefore not recommended. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Children less than 6 years of age: However safety and efficacy of valsartan in children aged 1 to 6 years have not been established.
Use in paediatric patients aged 6 to 18 years with renal impairment: Use in paediatric patients with a creatinine clearance <30 ml/min and paediatric patients undergoing dialysis has not been studied, therefore valsartan is not recommended in these patients. No dose adjustment is required for paediatric patients with a creatinine clearance >30 ml/min. Renal function and serum potassium should be closely monitored.
Use in paediatric patients aged 6 to 18 years with hepatic impairment: As in adults, valsartan is contraindicated in paediatric patients with severe hepatic impairment, biliary cirrhosis and in patients with cholestasis. There is limited clinical experience with valsartan in paediatric patients with mild to moderate hepatic impairment. The dose of valsartan should not exceed 80 mg in these patients.
Paediatric heart failure and recent myocardial infarction: Valsartan is not recommended for the treatment of heart failure or recent myocardial infarction in children and adolescents below the age of 18 years due to the lack of data on safety and efficacy.
Method of administration: Valsartan may be taken independently of a meal and should be administered with water.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out